The kidney
The urinary system consists of the paired kidneys, the paired ureters, the bladder and the urethra.
Functions of the kidney are:
The kidney is a highly vascular organ and receives 25% of cardiac output. It filters water and various
small molecules from the blood and then turns the filtrate into urine by selective reabsorption and
secretion.
When cells utilise amino acids for fuel, they remove the amino (-NH2) group as ammonia NH3. Ammonia
is VERY TOXIC!! 10g/ml of ammonia in the blood may be fatal! This ammonia passes into the
bloodstream from which it is rapidly removed from the liver and converted into urea through a metabolic
pathway called the urea cycle (or ornithine cycle, because it involves an intermediate compound called
ornithine).
Note: Fish excrete their waste as ammonia, because ammonia is very soluble in water and is removed
across the gills. Mammals do not have enough water to waste in flushing away ammonia. The nitrogen is
not removed as nitrogen gas, because production of nitrogen gas would require too much energy.
Insects and birds remove their nitrogenous waste as uric acid crystals. Uric acid is of very low toxicity and
can be removed at high concentration with the minimum amount of water, allowing these creatures to
conserve water very effectively.
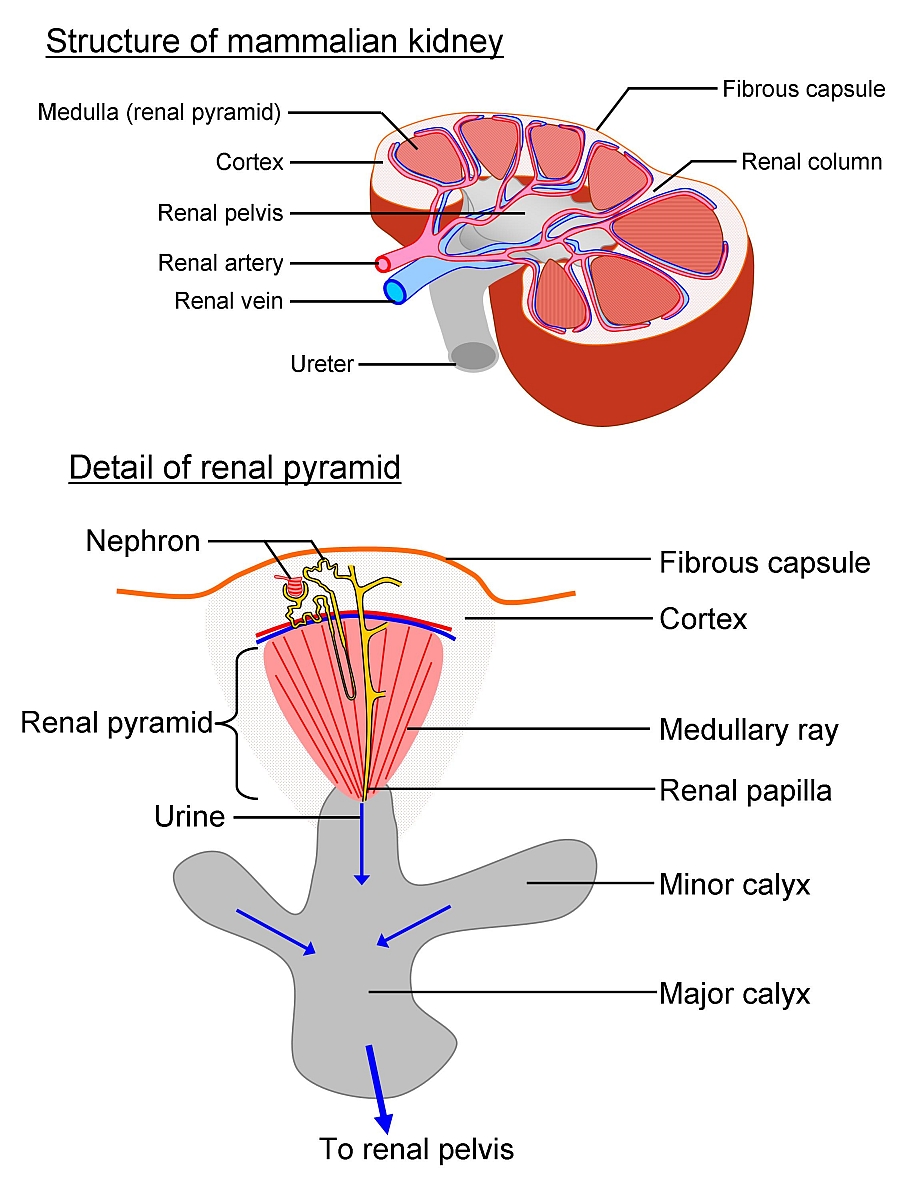
Each kidney is bean-shaped and about 10 cm long, 5 cm wide and 3 cm thick and weighs about 100g.
Each is divided into an outer cortex and an inner medulla (remember m for middle). Each is also divided
into about 12 wedge-shaped sectors called renal pyramids. The kidneys are located in the abdomen
against the back wall of the body. It is possible to function normally with one kidney, so there is reserve
capacity for times of severe water shortage.
The Nephron
The nephron is the functional unit of the kidney. Each kidney contains about 1 million nephrons.
Urine is produced in the nephrons by the processes of filtration and reabsorption.
The urinary system consists of the paired kidneys, the paired ureters, the bladder and the urethra.
Functions of the kidney are:
- To control the water and salt content of the body. (Water and salt content are linked by osmosis).
- Blood pH (acidity) regulation.
- Excretion of nitrogenous waste in the form of urea.
The kidney is a highly vascular organ and receives 25% of cardiac output. It filters water and various
small molecules from the blood and then turns the filtrate into urine by selective reabsorption and
secretion.
When cells utilise amino acids for fuel, they remove the amino (-NH2) group as ammonia NH3. Ammonia
is VERY TOXIC!! 10g/ml of ammonia in the blood may be fatal! This ammonia passes into the
bloodstream from which it is rapidly removed from the liver and converted into urea through a metabolic
pathway called the urea cycle (or ornithine cycle, because it involves an intermediate compound called
ornithine).
Note: Fish excrete their waste as ammonia, because ammonia is very soluble in water and is removed
across the gills. Mammals do not have enough water to waste in flushing away ammonia. The nitrogen is
not removed as nitrogen gas, because production of nitrogen gas would require too much energy.
Insects and birds remove their nitrogenous waste as uric acid crystals. Uric acid is of very low toxicity and
can be removed at high concentration with the minimum amount of water, allowing these creatures to
conserve water very effectively.
Each kidney is bean-shaped and about 10 cm long, 5 cm wide and 3 cm thick and weighs about 100g.
Each is divided into an outer cortex and an inner medulla (remember m for middle). Each is also divided
into about 12 wedge-shaped sectors called renal pyramids. The kidneys are located in the abdomen
against the back wall of the body. It is possible to function normally with one kidney, so there is reserve
capacity for times of severe water shortage.
The Nephron
The nephron is the functional unit of the kidney. Each kidney contains about 1 million nephrons.
Urine is produced in the nephrons by the processes of filtration and reabsorption.
Filtration (ultrafiltration)
Filtration occurs in the renal corpuscle (which is about 0.2 mm diameter) which consists of Bowman’s
capsule and the glomerulus. The glomerulus is a knot of capillaries embedded in the glomerulus. The
inner surface of the glomerulus encloses the glomerular capillaries and surrounds them completely.
Blood entering the glomerulus is at an exceptionally high pressure. This causes fluid in the blood to be
squeezed out of the glomerulus and into Bowman’s capsule. About 20% of the blood plasma entering the
glomerulus is filtered out of the capillaries into Bowman’s space (a space between the two layers of
Bowman’s capsule).
The glomerular capillary walls have large pores, or fenestrae (singular fenestra), that allow fluid and
small molecules to easily move out of the capillaries. The inner glomerular lining that surrounds these
capillaries is also composed of special cells called podocytes. Podocytes (‘foot cells’) have cytoplasmic
processes ending in pedicels (‘feet’) that sit on the basement membrane between the glomerular
capillary wall and the podocytes. Slits, about 25nm wide occur between the pedicels. Thus, both the
capillary wall and the glomerular inner lining are porous. The glomerular filtrate (or ultrafiltrate)
contains small molecules, like glucose, amino acids and vitamins, but lacks the large molecules like
proteins. These large proteins can not cross through the fenestrae and podocyte slit pores.
The glomerular filtrate flows into the proximal convoluted tubule, where selective reabsorption first takes
place. The glomerular filtration rate (GFR) is the volume of fluid entering the tubule per unit time.
Filtration occurs in the renal corpuscle (which is about 0.2 mm diameter) which consists of Bowman’s
capsule and the glomerulus. The glomerulus is a knot of capillaries embedded in the glomerulus. The
inner surface of the glomerulus encloses the glomerular capillaries and surrounds them completely.
Blood entering the glomerulus is at an exceptionally high pressure. This causes fluid in the blood to be
squeezed out of the glomerulus and into Bowman’s capsule. About 20% of the blood plasma entering the
glomerulus is filtered out of the capillaries into Bowman’s space (a space between the two layers of
Bowman’s capsule).
The glomerular capillary walls have large pores, or fenestrae (singular fenestra), that allow fluid and
small molecules to easily move out of the capillaries. The inner glomerular lining that surrounds these
capillaries is also composed of special cells called podocytes. Podocytes (‘foot cells’) have cytoplasmic
processes ending in pedicels (‘feet’) that sit on the basement membrane between the glomerular
capillary wall and the podocytes. Slits, about 25nm wide occur between the pedicels. Thus, both the
capillary wall and the glomerular inner lining are porous. The glomerular filtrate (or ultrafiltrate)
contains small molecules, like glucose, amino acids and vitamins, but lacks the large molecules like
proteins. These large proteins can not cross through the fenestrae and podocyte slit pores.
The glomerular filtrate flows into the proximal convoluted tubule, where selective reabsorption first takes
place. The glomerular filtration rate (GFR) is the volume of fluid entering the tubule per unit time.
Reabsorption
Reabsorption occurs in the nephron tubules and is the process whereby materials in the filtrate are
selectively reabsorbed, that is taken up from the filtrate in the tubule lumen by the tubule epithelial cells
and passed into the extracellular tissue space where they are taken up by blood capillaries. All glucose,
most amino acids and water-soluble vitamins are reabsorbed (since these are useful to the body!). The
reabsorption of water and salts is controlled.
Proximal convoluted tubule
The proximal convoluted tubule is the longest part of the nephron and reabsorbs more than 2/3 of the
water from the filtrate.
Here the glucose, amino acids and vitamins are all reabsorbed. Glucose and amino acids are actively
reabsorbed (i.e. their absorption requires energy from ATP) along with sodium ions. The pumping of
sodium ions out of the tubule lumen (sodium ion reabsorption) is driven by sodium pumps that require
ATP. Transport molecules couple this transport of sodium to the transport of glucose and amino acids.
Negatively charged chloride ions (Cl-), bicarbonate ions (HCO3-) and phosphate ions (PO43-) follow the
sodium (attracted to the positive charge). Water also follows this movement of ions and sugars, driven by
osmosis. Thus sodium pumping drives the movements of negative ions and glucose, etc. out of the
tubule lumen.
The epithelial cells forming the wall of the proximal tubule are cuboidal and have many microvilli
projecting into the tubule lumen. These microvilli increase their surface area for reabsorption. They
contain many mitochondria to provide the ATP needed for sodium pumping.
Loop of Henle
The descending limb of the loop of Henle (thin part) has a thinner epithelium with no microvilli and has
few mitochondria, and so is metabolically less active than the proximal tubule epithelium. Water passively
moves out of the descending limb by osmosis, into the salt-rich surrounding tissue.
The ascending limb of the loop of Henle has a thicker epithelium and more mitochondria and actively
reabsorbs sodium ions (and so chloride ions too). It secretes hydrogen ions into the tubule lumen (part
of blood acid-level regulation).
The loop of Henle is a countercurrent multiplier
The flows in the ascending and descending loops of Henle are in opposite directions (a countercurrent).
This arrangement increases the concentration of salt (the osmolarity – which is the amount of solute (like
salt) per unit volume of water) in the medulla and also causes the salt concentration in the medulla to
increase with distance from the cortex.
The water is eventually taken up by blood capillaries surrounding the loop of Henle. This capillary
network is called the vasa recta. Thus, water is conserved, otherwise we would dehydrate by urine loss!
Some water must remain, however, to carry away the waste urea and excess water.
Note: the length of the loop of Henle and how far it penetrates into the medulla determine the amount of
water reabsorbed in the loop. Some nephrons have short loops, others have long loops. Those with long
loops function in times of water shortage and conserve water by increasing water reabsorption from the
filtrate. Animals adapted to desert conditions have longer loops of Henle. Desert rats are so efficient at
reabsorbing water from their urine that they do not need to drink ever! They obtain all their water from
(dry) food and from respiration!
Distal convoluted tubule
The distal convoluted tubule contains cuboidal epithelium, but with fewer microvilli than the proximal
tubule, and so is less active in reabsorption. However, some Na+ and Cl- are reabsorbed. Protons (H+,
hydrogen ions) and ammonia are secreted by the distal tubule epithelium into the tubule lumen. These
combine to form ammonium ions (NH4+). This process is part of acidity (pH) regulation, since the
ammonium is passed out in the urine, taking excess acid (protons account for acidity!) with it.
Collecting duct
Several nephrons share the same collecting duct. The collecting ducts collect the filtrate and pass it into
the calyces of the kidney and hence into the renal pelvis and on into the ureter. The (pair of) ureters
(one from each kidney) are narrow muscular tubes that pass the filtrate (now urine rich in urea) to the
bladder. (The peristaltic waves of muscular constriction in the ureters pump the urine down the ureters).
When the bladder is about one-third full, stretch receptors in the bladder wall tell the brain of the need to
evacuate the bladder! The bladder connects to the outside via a tube called the urethra.
However, during passage of the filtrate along the collecting ducts a very important process occurs. The
collecting duct is permeable to water and so water leaves the ducts, by osmosis, into the salty medulla.
Some urea also diffuses out, contributing to the high osmolarity of the medulla. (Remember that this high
osmolarity draws water out of the descending loop of Henle and the collecting duct). This means that by
the time that the urine passes out of the collecting duct into the calyx, it is hypertonic (i.e. saltier than
blood plasma, and especially rich in urea).
Furthermore, the collecting duct has its permeability to water controlled. When the body is hydrated with
excess water, then large amounts of dilute urine are produced, by reducing the permeability of the
collecting ducts to water. When the body is dehydrated, then the permeability of the collecting ducts to
water is increased, so that more water leaves the urine and the urine is more concentrated and less in
quantity – conserving water.
The permeability of the collecting ducts to water is regulated by antidiuretic hormone (ADH).
When the body is short of water:
When the body has excess water:
(Note: The juxtaglomerular apparatus consists of part of the afferent and efferent arterioles and part
of the distal convoluted tubule. (Juxta: next to, ‘juxtaglomerular’ means ‘next to the glomerulus’). The
juxtaglomerular apparatus of the nephron secretes the hormone renin (one of the endocrine functions of
the kidney). Renin increases blood pressure in the body if the filtration rate in the kidney is too low.
Renin causes the arterioles supplying each glomerulus to constrict (become narrower). This increases
blood pressure in the glomerulus and so increases the GFR).
Kidney histology: https://histo.life.uiuc.edu/histo/atlas/oimages.php?oid=1215
Reabsorption occurs in the nephron tubules and is the process whereby materials in the filtrate are
selectively reabsorbed, that is taken up from the filtrate in the tubule lumen by the tubule epithelial cells
and passed into the extracellular tissue space where they are taken up by blood capillaries. All glucose,
most amino acids and water-soluble vitamins are reabsorbed (since these are useful to the body!). The
reabsorption of water and salts is controlled.
Proximal convoluted tubule
The proximal convoluted tubule is the longest part of the nephron and reabsorbs more than 2/3 of the
water from the filtrate.
Here the glucose, amino acids and vitamins are all reabsorbed. Glucose and amino acids are actively
reabsorbed (i.e. their absorption requires energy from ATP) along with sodium ions. The pumping of
sodium ions out of the tubule lumen (sodium ion reabsorption) is driven by sodium pumps that require
ATP. Transport molecules couple this transport of sodium to the transport of glucose and amino acids.
Negatively charged chloride ions (Cl-), bicarbonate ions (HCO3-) and phosphate ions (PO43-) follow the
sodium (attracted to the positive charge). Water also follows this movement of ions and sugars, driven by
osmosis. Thus sodium pumping drives the movements of negative ions and glucose, etc. out of the
tubule lumen.
The epithelial cells forming the wall of the proximal tubule are cuboidal and have many microvilli
projecting into the tubule lumen. These microvilli increase their surface area for reabsorption. They
contain many mitochondria to provide the ATP needed for sodium pumping.
Loop of Henle
The descending limb of the loop of Henle (thin part) has a thinner epithelium with no microvilli and has
few mitochondria, and so is metabolically less active than the proximal tubule epithelium. Water passively
moves out of the descending limb by osmosis, into the salt-rich surrounding tissue.
The ascending limb of the loop of Henle has a thicker epithelium and more mitochondria and actively
reabsorbs sodium ions (and so chloride ions too). It secretes hydrogen ions into the tubule lumen (part
of blood acid-level regulation).
The loop of Henle is a countercurrent multiplier
The flows in the ascending and descending loops of Henle are in opposite directions (a countercurrent).
This arrangement increases the concentration of salt (the osmolarity – which is the amount of solute (like
salt) per unit volume of water) in the medulla and also causes the salt concentration in the medulla to
increase with distance from the cortex.
- The descending loop is impermeable to salt, but is permeable to water.
- The ascending loop is impermeable to water but reabsorbs sodium ions (and chloride ions) and
pumps them into the medulla tissue. - This pumping of salt by the ascending loop increases the salt concentration in the medulla and
causes water to leave the descending loop by osmosis. - Filtrate at the bottom of the loop of Henle is now hypertonic to blood plasma (i.e. contains more
salt). This makes it easier for salt to be reabsorbed from the ascending loop (especially in the first
part of the ascending loop) which enhances the salt concentration in the medulla and so enhances
(multiplies) the reabsorption of water in the descending loop.
The water is eventually taken up by blood capillaries surrounding the loop of Henle. This capillary
network is called the vasa recta. Thus, water is conserved, otherwise we would dehydrate by urine loss!
Some water must remain, however, to carry away the waste urea and excess water.
Note: the length of the loop of Henle and how far it penetrates into the medulla determine the amount of
water reabsorbed in the loop. Some nephrons have short loops, others have long loops. Those with long
loops function in times of water shortage and conserve water by increasing water reabsorption from the
filtrate. Animals adapted to desert conditions have longer loops of Henle. Desert rats are so efficient at
reabsorbing water from their urine that they do not need to drink ever! They obtain all their water from
(dry) food and from respiration!
Distal convoluted tubule
The distal convoluted tubule contains cuboidal epithelium, but with fewer microvilli than the proximal
tubule, and so is less active in reabsorption. However, some Na+ and Cl- are reabsorbed. Protons (H+,
hydrogen ions) and ammonia are secreted by the distal tubule epithelium into the tubule lumen. These
combine to form ammonium ions (NH4+). This process is part of acidity (pH) regulation, since the
ammonium is passed out in the urine, taking excess acid (protons account for acidity!) with it.
Collecting duct
Several nephrons share the same collecting duct. The collecting ducts collect the filtrate and pass it into
the calyces of the kidney and hence into the renal pelvis and on into the ureter. The (pair of) ureters
(one from each kidney) are narrow muscular tubes that pass the filtrate (now urine rich in urea) to the
bladder. (The peristaltic waves of muscular constriction in the ureters pump the urine down the ureters).
When the bladder is about one-third full, stretch receptors in the bladder wall tell the brain of the need to
evacuate the bladder! The bladder connects to the outside via a tube called the urethra.
However, during passage of the filtrate along the collecting ducts a very important process occurs. The
collecting duct is permeable to water and so water leaves the ducts, by osmosis, into the salty medulla.
Some urea also diffuses out, contributing to the high osmolarity of the medulla. (Remember that this high
osmolarity draws water out of the descending loop of Henle and the collecting duct). This means that by
the time that the urine passes out of the collecting duct into the calyx, it is hypertonic (i.e. saltier than
blood plasma, and especially rich in urea).
Furthermore, the collecting duct has its permeability to water controlled. When the body is hydrated with
excess water, then large amounts of dilute urine are produced, by reducing the permeability of the
collecting ducts to water. When the body is dehydrated, then the permeability of the collecting ducts to
water is increased, so that more water leaves the urine and the urine is more concentrated and less in
quantity – conserving water.
The permeability of the collecting ducts to water is regulated by antidiuretic hormone (ADH).
When the body is short of water:
- Osmoreceptors in the hypothalamus detect the drop in body water as the body fluids become
saltier. The receptors increase their activity, stimulating the pituitary gland to release more ADH.
This ADH increases the permeability of the collecting ducts to water and so increases water
reabsorption and reduces the quantity of water in the urine, thus reducing water loss. Thus, a
smaller quantity of more concentrated urine is produced. - Thirst receptors in the thalamus (part of the brain) also detect the increased osmolarity of bodily
fluids and make us feel thirsty. - Stretch receptors (pressure receptors or baroreceptors) in the carotid sinus in each carotid artery
in the neck, and at the junction between veins and the atria of the heart, measure the drop in
blood volume (which causes a drop in blood pressure) and stimulate increased release of ADH. - The sympathetic nervous system causes blood vessels to constrict, increasing blood pressure to
its normal value (if possible!).
When the body has excess water:
- The osmoreceptors in the hypothalamus detect the drop in osmolarity of body fluids (as they
become more dilute) and reduce secretion of ADH from the pituitary. Thus, the permeability of the
collecting ducts to water is reduced, thus reducing water reabsorption in the collecting ducts, and
a larger quantity of more dilute urine is produced, expelling the excess water from the body. - Thirst receptors stop firing, so we stop feeling thirsty.
- Pressure receptors detect the rise in blood volume/pressure and stop stimulating ADH secretion.
- The parasympathetic nervous system causes blood vessels to widen (dilate) to lower blood
pressure to its normal value.
(Note: The juxtaglomerular apparatus consists of part of the afferent and efferent arterioles and part
of the distal convoluted tubule. (Juxta: next to, ‘juxtaglomerular’ means ‘next to the glomerulus’). The
juxtaglomerular apparatus of the nephron secretes the hormone renin (one of the endocrine functions of
the kidney). Renin increases blood pressure in the body if the filtration rate in the kidney is too low.
Renin causes the arterioles supplying each glomerulus to constrict (become narrower). This increases
blood pressure in the glomerulus and so increases the GFR).
Kidney histology: https://histo.life.uiuc.edu/histo/atlas/oimages.php?oid=1215
| | | | | | |


| Excretion |

